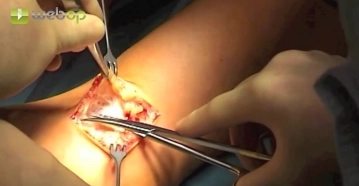
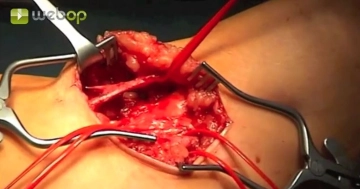
Locate and dissect the cephalic vein, which is encircled centrally with a vessel loop. Close off the vein peripherally by simple ligation approximately 1 cm distal to the junction of the side branch. Occlude the vein centrad with a soft bulldog clamp and take down both the vein and its lateral branch peripherally. Carry the incision of the vein into the lateral branch, resulting in a flared shape.
After careful dilation probe the cephalic vein centrad with a Fogarty catheter to verify venous patency in the upper arm. Delicately dilate the vein when withdrawing the catheter. Administer 1000 IU of heparin saline solution centrad
Tips:
1. Do not bruise the vein with the forceps.
2. If the peripheral vein is supplied by a suitable collateral branch, use it fashion a flared anastomosis. This will facilitate the anastomosis.
3. In case of small vein caliber, carefully dilate the cephalic vein along the entire course on the upper arm with a balloon catheter.