
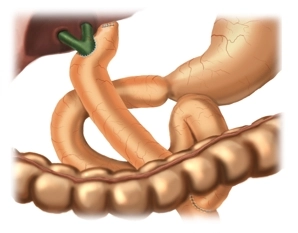
In the high-hilar Hepatico-Jejunostomy according to Hepp-Couinaud, the anastomosis of the Roux jejunal loop with the extrahepatic left hepatic duct is performed side-to-side. This high form of biliodigestive anastomosis is chosen for strictures that extend to the bifurcation but with preserved confluence.
Otherwise, the surgical technique is similar to the anastomosis technique, biliodigestive, classic.
- A wide anastomotic opening should be created as much as possible.
- The suture with single-layer full-thickness interrupted sutures should be primarily tight.
- An exact adaptation of the bile and intestinal mucosa must be aimed for.