- Terminal renal insufficiency with planned peritoneal dialysis
-
Indications
-
Contraindications
- Patient is not suitable for peritoneal dialysis
- Cystic kidneys filling the abdomen
-
Preoperative Diagnostics
- Clinical examination: Abdominal wall hernia? Previous abdominal operations?
- Abdominal sonography: Exclusion of tumors, assessment of the size of cystic kidneys and renal cysts.
-
Special Preparation
![Special Preparation]()
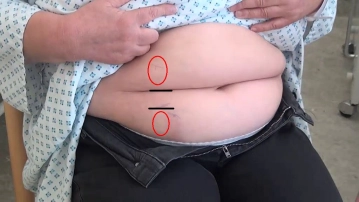
Sitting position: possible catheter exits marked in red outside of waistbands and skin folds
1 week preoperatively
- No more heparin or insulin injections in the area of the abdominal wall to spare the surgical area and reduce the risk of infection
Day before surgery
- Usual surgical preparation with navel care
- Enema on the evening before
- Last meal on the evening before
- Preoperative marking on the standing and sitting patient
Since CAPD is performed by the patient themselves, the catheter exit site must be easily visible to them. Therefore, the exit site must not be located at the level of the waistband (upper and lower clothing), skin folds, or below an apron of fat. Since patients usually perform the dialysate exchange while sitting, the intended exit site should also be checked preoperatively while sitting. The side localization, right or left, should be left open preoperatively, as any existing intraoperative adhesions may be decisive for this.
Surgery day
- Single-shot antibiotic before induction of anesthesia
- If necessary, urinary catheter for the duration of the operation
-
Informed Consent
- Primary laparoscopy with assessment of the abdominal cavity
- If necessary, laparoscopic adhesiolysis
Complications
- Injury to small or large intestine
- Injury to parenchymal organs
- Wound infection, abscess, peritonitis; subsequent interventions
- Abdominal wall hematoma, subcutaneous emphysema
- Postoperative shoulder pain
- Thromboembolism
Specific Catheter Complications
- Catheter kinking
- Catheter malposition, leakages
Postoperative Behavioral Instructions
- 2 days strict bed rest
- 2 days getting up only to go to the toilet
Anesthesia
Intubation anesthesia in capnoperitoneum ... - Operations in general, visceral and transplant surge
Intubation anesthesia in capnoperitoneum ... - Operations in general, visceral and transplant surge
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.08 / module
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.17
/ month
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.