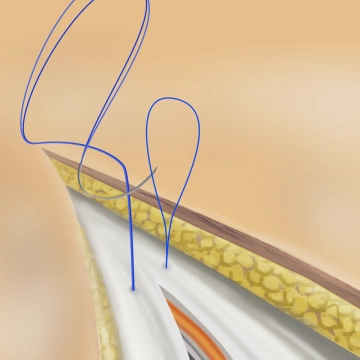
The surgeon grasps the fascia with the surgical forceps and pierces through the fascia 1 cm from the edge with a twisting motion. Both the anterior and posterior fascial layers are grasped together.
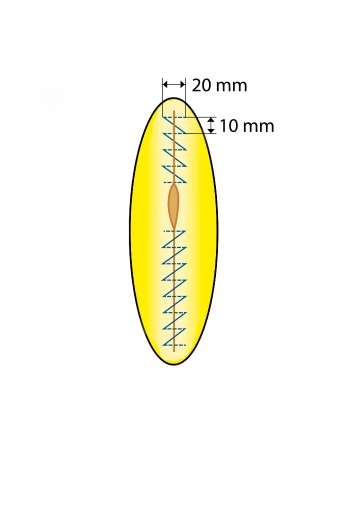
The first stitch is placed approximately 1 cm cranial to the end of the wound to anchor the loop in the non-incised fascial area. The insertion is V-shaped from the healthy tissue into the incision and from the incision into the healthy tissue. The needle is pulled through the loop and the suture is then performed in a continuous technique. The loop is sutured from the wound edge to the wound center. The distance between the stitches is about 1 cm, achieving a thread-to-wound length ratio of at least 4:1. The cranial suture line is continued to the middle of the incision.
Note: In fascial suturing, only the aponeurosis should be grasped, as muscle in the stitch area can become necrotic and lead to loosening of the fascial closure.
The peritoneum is not closed separately but can be included.
Peritoneal bulges in the suture line should be avoided.