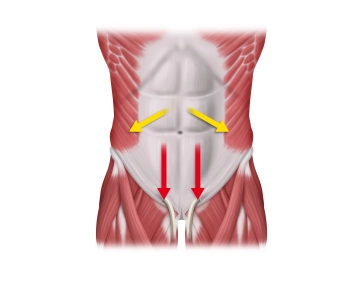
The strongly segmental character of the thoracic wall's structure continues in a weakened form into the abdomen, but decreases from cranial to caudal. Since the segmental character of the ventral abdominal wall is particularly pronounced in the upper portion, forces in this area act mainly in a mediolateral direction. Median incisions result in a stronger centrifugal pull on the fascial edges than transverse incisions. Below the navel, longitudinal stress becomes more prominent, so the lateral pull on the fascial edges is less with longitudinal incisions, which is why the abdominal wall above the navel is more prone to dehiscence than the lower portion. The closure of median laparotomy is associated with high tensile stresses and could, among other things, explain the high number of postoperative incisional hernias.
-
Anatomical and Functional Characteristics of the Anterior Abdominal Wall
![Anatomical and Functional Characteristics of the Anterior Abdominal Wall]()
-
Aspects of Surgical Wound Closure in Laparotomy
The restored abdominal wall with a mechanically stable and cosmetically satisfactory healed laparotomy wound is a visible expression of a successful operation.
Good fascial healing is achieved not through a lot of scar tissue, but rather through minimal and well-matured scar tissue. This corresponds to the surgical demand for gentle technique, avoidance of wound infections, and high suture tensions. Incisional hernias represent the most common long-term complication after laparotomy.
Optimizing fascial healing is the prophylaxis of incisional hernia. The prerequisite is the understanding of fascial suturing as merely temporary support for local wound healing processes. During the exudative phase (days 1-4), there is no tensile strength of the wound. In the proliferative phase (days 5-20), granulation tissue is developed, creating a new connective tissue matrix, which, however, initially only exhibits 15-30% of the original tensile strength. This process can be significantly delayed by a hematoma or infection in the wound. The necessary formation of scar tissue should not be viewed as static but as a permanent remodeling of the abdominal wall even after years.
The continuous, all-layer abdominal wall closure with a suture-to-wound length ratio of at least 4:1 using monofilament, late-absorbable thread is superior to the single interrupted suture technique. Its advantage is better biomechanics with favorable collagen synthesis in the incision area, as well as the economic aspect of significant time and material savings. Biomechanically, the distribution of suture tension on small tissue bridges seems to be crucial.
During closure, attention should be paid to adequate tension of the continuous suture that adapts the fascial edges with minimal stress on the tissue bridges to prevent "buttonholes" as initiators of incisional hernia.
Additionally, the elasticity of the suture material, corresponding to the physiological excursions of the abdominal wall, is another factor in preventing the formation of "buttonholes".
-
The Suture Material
During healing, the abdominal wall is subjected to various stresses. The suture must absorb some of the forces generated in the process. Ideally, this suture should have rubber-elastic properties. The repair phase of the abdominal wall takes about three months to reach 75 percent of the original tissue strength. The loss of tensile strength of the suture should be adapted to the healing of the abdominal wall.
A slowly absorbable suture is the ideal suture material. The use of non-absorbable sutures does reduce the incidence of incisional hernias but is associated with significantly more local complications such as suture fistulas and prolonged wound pain.
The suture used in the article, MonoMax®, is a new generation suture material made from poly-4-hydroxybutyrate. MonoMax® is a monofilament suture with high tensile strength that physically supports the abdominal wall for six months and is fully absorbed after one year. It is characterized by ultra-late absorption, high elasticity, and high flexibility. In particular, the elasticity reduces the cutting of the stitch channels to the fascial edges and spares the tissue.
The currently favored loop sutures have the advantage that one of the knots in the wound corners can be omitted.
The method of choice for secure fascial closure is currently the continuous closure with a loop sut
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
US$85.05/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$170.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.