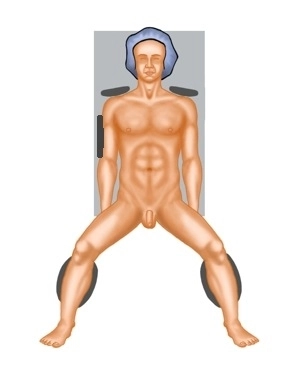
Ideally, positioning is done in lithotomy position on a large vacuum cushion (on the right side, the cushion supports the rib cage and iliac crest to prevent the patient's weight in right lateral position from pressing on the arm).
Additionally, sufficient support of the shoulders must be ensured to prevent slipping during prolonged Trendelenburg and right lateral positioning.
It is recommended to position both arms (caution: cotton wrapping when positioning with a cloth sling).
Cotton wrapping of the knees and proximal lower legs is also performed to prevent pressure injuries.
For leg positioning, padded "boots" are recommended for optimal cushioning with separate sterile draping of the legs. Alternatively, the legs can be positioned in leg holders with fixation in these.
The legs should be adjustable in flexion and extension via the OR table control.
Note: Before sterile washing, always test the positioning in Trendelenburg and right lateral position with the remote control.
Caution: Vacuum cushions may have leaks. Therefore, they should be checked again before sterile draping.