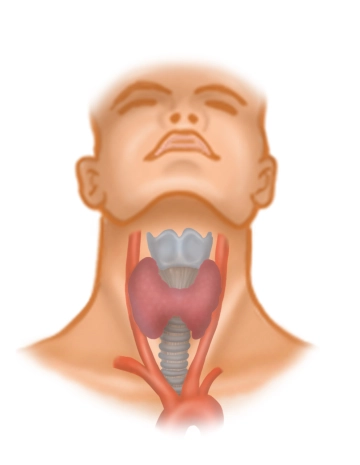
Located between the anterior border of the M. sternocleidomastoideus, the mandible, and the jugular fossa, the anterior neck triangle in the area of the hyoid bone includes the supra- and infrahyoid musculature, vessels, nerves, and the thyroid gland. For thyroidectomy, among the infrahyoid muscles, possibly the medially located
- M. sternohyoideus (sternum → hyoid bone) and below it the
- M. sternothyroideus (sternum → thyroid cartilage of the larynx) as well as further laterally the
- M. omohyoideus (scapula → intermediate tendon → hyoid bone)
are of importance, as they partially cover the thyroid gland and must be pushed aside intraoperatively.
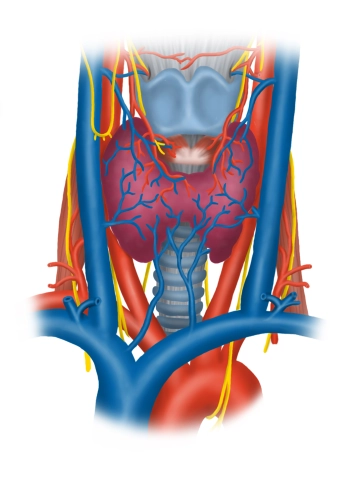
Blood Vessels
The common carotid artery divides at the upper edge of the thyroid cartilage at the level of its carotid sinus (receptors for blood pressure and chemoreceptors for blood gases) into its internal and external branches and runs previously immediately lateral in the carotid sheath next to the trachea and esophagus cranially. Here it touches as a large vessel the right and left thyroid lobes. From the sigmoid sinus of the skull emerges the internal jugular vein, which collects blood from the skull and neck, pulling caudally first adjoining the internal carotid artery in the carotid sheath, then running further laterally and enclosing the common carotid artery as well as the vagus nerve (X) laterally.
Nerves
In addition to the vagus nerve and its upper branch to the larynx (N. laryngeus superior → M. cricothyroideus anterior, as well as mucosa of the upper larynx half), located in the area of the thyroid gland laterally, descending from above, is the ansa cervicalis profunda (superior and inferior roots, from C1-C3) for the innervation of the three mentioned muscles of the anterior neck triangle and the N. transversus colli (from C2/3, skin innervation, platysma).
Fascial Layers
In the anterior neck triangle, several fascial layers (all belonging to the cervical fascia) are located under the skin, which exhibit certain peculiarities:
- The superficial lamina superficialis surrounds all neck structures except for the platysma and separately envelops the M. sternocleidomastoideus and dorsally the M. trapezius (N. accessorius XI),
- the middle lamina pretrachealis surrounds the infrahyoid musculature, and the
- deep lamina prevertebralis runs between the esophagus and the spine outside the surgical area.
The thyroid gland/parathyroid glands and the trachea possess, just like the lateral vessel-nerve bundle (A. carotis, V. jugularis interna, and N. vagus), in addition their own organ fascias. Due to the arrangement of the cervical fascias, compartments enclosed by them and spaces in between (spatia) arise, which extend into the mediastinum and represent potential infection pathways.