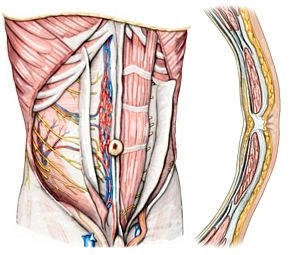
1. Anterior Abdominal Muscles
M. rectus abdominis: straight abdominal muscle within the rectus sheath with 3-4 tendinous transverse stripes (Intersectiones tendineae), which are fused with the anterior leaf of the rectus sheath.
M. pyramidalis: originates from the upper pubic ramus and radiates into the linea alba, lies ventral to the M. rectus abdominis in its own sheath in the anterior leaf of the rectus sheath.
2. Layer Structure of the Anterior Abdominal Wall
Rectus Sheath: encloses the M. rectus abdominis; above the midpoint between the umbilicus and symphysis, an anterior and posterior leaf are distinguished; the posterior leaf ends here in the form of the linea arcuata; above this line, the M. obliquus externus abdominis radiates into the anterior leaf of the rectus sheath, the M. obliquus internus abdominis into the anterior and posterior leaf, and the M. transversus abdominis into the posterior leaf.
Linea semilunaris: transition zone between the aponeuroses of the lateral abdominal muscles and the lateral edge of the rectus sheath.
Linea alba: approximately 1 cm wide taut connective tissue strip between the right and left rectus sheath, extends from the sternum to the symphysis.
Fascia transversalis: above the linea arcuata, it covers the posterior leaf of the rectus sheath internally, below the linea it lies directly on the M. rectus abdominis.
3. Internal Relief of the Abdominal Wall
Plica umbilicalis mediana: median peritoneal fold that runs from the umbilicus to the urinary bladder, within the fold is the Lig. umbilicale medianum (connective tissue strand = urachus remnant).
Plica umbilicalis medialis: paired peritoneal fold, contains on both sides the Lig. umbilicale mediale = obliterated remnant of the bilateral umbilical artery, A. umbilicalis.
Plica umbilicalis lateralis: paired peritoneal fold, beneath it lies on both sides the A. epigastrica inferior with two accompanying veins each.
4. Conduction Pathways
a) Arteries
A. epigastrica superior: continuation of the A. thoracica interna, anastomoses at umbilical level with the A. epigastrica inferior.
A. epigastrica inferior: arises from the A. iliaca externa and runs like the aforementioned artery on the dorsal surface of the M. rectus abdominis in the rectus sheath.
A. epigastrica superficialis: originates from the A. femoralis and distributes after crossing the inguinal ligament in the subcutaneous tissue of the anterior abdominal wall.
Aa. intercostales posteriores VI – XI and A. subcostalis: originate from the thoracic aorta; their terminal segments run obliquely downward between M. obliquus internus abdominis and M. transversus abdominis and proceed from lateral to the rectus sheath, where they anastomose with A. epigastrica superior et inferior.
b) Veins
Vv. epigastricae superiores: accompany the artery of the same name; anastomose with branches of the V. epigastrica inferior and drain into the Vv. thoracicae internae.
V. epigastrica inferior: branches into accompanying veins of the A. epigastrica inferior and drains into the V. iliaca externa.
V. epigastrica superficialis: runs parallel to the artery of the same name (see above).
c) Lymphatic Vessels
Superficial Lymphatic Vessels: above the umbilicus, they drain to the axillary lymph nodes (Nodi lymphatici axillaris) below to the inguinal lymph nodes, Nodi lymphatici inguinales.
Deep Lymphatic Vessels: generally run parallel to the blood vessels; reach the Nodi lymphatici parasternales, lumbales, and iliaci externi.
d) Nerves
Nn. intercostales VI – XII: as Rr. ventrales of the Nn. thoracici VI – XII; they enter the abdominal wall behind the costal cartilages between M. obliquus internus abdominis and M. transversus abdominis; motor branches supply the anterior and lateral abdominal muscles, the sensory branches the abdominal skin.
N. iliohypogastricus, N. ilioinguinalis and N. genitofemoralis: participate in the motor and sensory innervation of the lower abdominal region and genitals.