
The CT scan shows a dislocated metaphyseal fracture of the distal radius with an additional ulno-palmar key fragment as well as a shell-shaped avulsion of the dorsal radius rim.
-
Planning the Operation
Soundsettings -
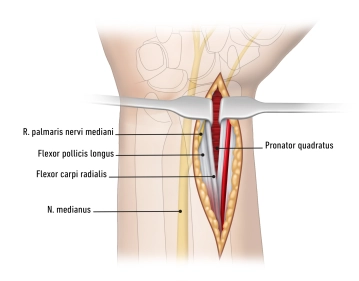
Approach modified according to Henry
![Approach modified according to Henry]()
Soundsettings Radio-palmar access to the distal radius radial to the tendon of the M. flexor carpi radialis from the distal palmar crease approximately 8-10 cm proximally. Preparation through the antebrachial fascia at the level of the tendon sheath. In doing so, the A. radialis and, by displacing all finger flexor tendons ulnarly, the N. medianus including the palmar branch of the median nerve are safely spared.
The M. pronator quadratus is transected transversely to the fiber direction in the area of its radial attachment and prepared in its entirety from the palmar surface of the radius as an ulnarly pedicled flap.
Tip
A crossing of the flexion crease as well as an ulno-palmar approach should be absolutely avoided, as this is associated with a high incidence of scar contracture as well as injury to the palmar branch of the median nerve.
Guiding structures
- Distal palmar crease
- Tendon of the flexor carpi radialis
- N. medianus with palmar branch
- A. radialis
Reposition
The plate bed is exposed subperiosteally at the distal radius, without opening the periosteal tube.
The plate bed is exposed subperiosteally at the distal radius, without opening the periosteal tube.
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.26 / module
US$51.22/ yearly payment
hand surgery
Unlock all courses in this module.
US$8.53
/ month
US$102.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.