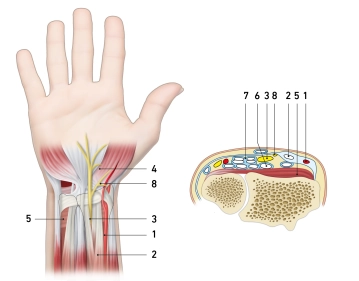
- Radial artery
- Tendon of the flexor carpi radialis muscle
- Median nerve
- Thenar branch of the median nerve
- Pronator quadratus muscle
- Tendon of the flexor digitorum profundus muscle
- Tendon of the flexor digitorum superficialis muscle
- Palmar branch of the median nerve
Modified Henry Approach
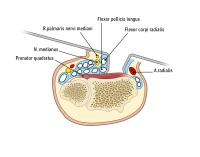
The modified Henry approach is suitable for exposing most fractures of the distal radius. While the classic Henry approach is between the radial artery and the brachioradialis muscle, the modified Henry approach involves longitudinally splitting the tendon sheath of the flexor carpi radialis muscle and entering between it and the radial artery. The modified approach is comfortable and low in complications, however, the radial artery and the palmar cutaneous branch of the median nerve are at risk.
Plate Design
The development of angle-stable plate systems has led to a change in the surgical treatment of distal radius fractures. Whereas previously the predominant technique was dorsal buttress plate osteosynthesis, today palmar angle-stable plate osteosynthesis represents the gold standard.
Due to the widespread use of this technique, a variety of different plate systems are now available, which exhibit significant differences that must be considered when selecting them. These relate to the plate design and the various locking techniques.
The VariAx™ plate from Stryker used here is side-specific, takes into account the curved structure of the radius and shows the traditional T-shape. The distal edge of the transverse arm is shaped to match the so-called watershed line of the distal radius, a theoretical line that marks the most palmar aspect of the palmar edge of the radius. This line runs distal to the pronator quadratus line and is covered by the palmar capsule.
When positioning the plate distal to the watershed line, the contact pressure on the flexor tendons increases significantly depending on the extension position of the wrist. The tendon of the flexor pollicis longus muscle (FPL) is exposed to the highest pressures, most likely due to its location and course. Studies have shown that plates placed palmar to this line serve as a pivot point for the flexor tendons - especially during wrist extension. This makes (peri)tendinitis or tendon rupture, especially of the flexor pollicis longus tendon, highly likely.

Two distal screw rows allow high flexibility in screw positioning, which is advantageous in the presence of osteoporosis or multifragment fractures. Both central and dorsal articular surfaces can be optimally captured with this, the subchondral position of the screws prevents secondary dislocation. The screw holes are designed in such a way that multidirectional, angle-stable anchoring of the screws with a range of 15° is possible. The screw heads are recessed in the plate and do not protrude. Together with the flat plate design (low-profile) and the watershed shape, they help to prevent rupture of the flexor tendons.
The longitudinal arm of the plate allows dynamic correction of the plate position during reduction through the gliding hole in the middle. Proximal and distal to it, the plate can be securely fixed with additional angle-stable screws.