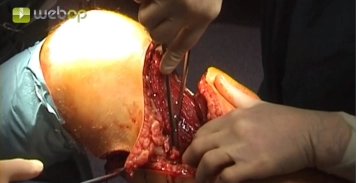
Fishmouth incision down to the fascia at the transition from the middle to the distal third of the thigh. Divide the great saphenous vein between ligatures (not shown in video). Insert the long amputation knife laterally at the angle of the incision, down to the femur, sliding on the femur anterially, and exiting medially at the posterior border of the quadriceps. Fashion the anterior skin-muscle flap by swiftlytransecting the musculature anteriorly along the incision in one motion with the amputation knife. In doing so, manually pre-stretch the quadriceps.
Tip:
1. The interface between the anterior and posterior flaps is formed by the medial and lateral margins of the quadriceps muscle.
2. Short incisions (hacking) compromise wound healing. Transection should be rapid and smooth, as a swift, targeted approach will result in low blood loss.
3. Possibly mark the incision on the skin; center the angle of the fishmouth on the femur.