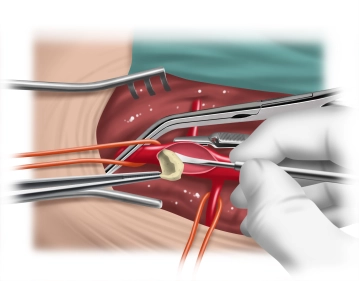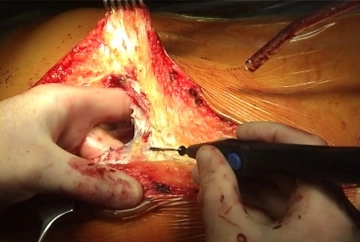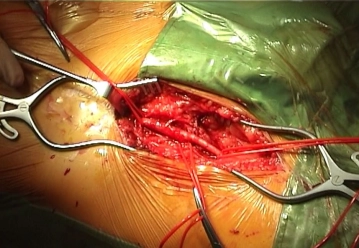
Longitudinal skin incision about 1 cm lateral to the femoral artery and transection of the subcutis with painstaking hemostasis. While sparing the lymphatics divide the lateral collectors immediately inferior to the groin between clamps and secure the ends by suture ligation. Dissect and loop the common, superficial, and deep femoral arteries Palpate the vessel walls (quality, calcification).
Tips:
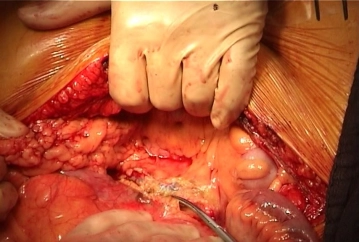
1. The first step is to expose the groin so that the abdominal cavity remains open only as briefly as possible. As a result, the patient cools down less quickly, which improves the postoperative phase and allows for faster extubation.
2. Lateral access to the femoral artery allows staggered closure of the groin. This better secures the vascular reconstruction, and superficial wound healing disorders, such as wound margin necrosis, do not necessarily result in deep infection.
3. Especially in PAOD Fontaine stage IV, the lymphatics and lymph nodes are often quite enlarged and represent a potential source of infection in vascular surgery Careful instrument dissection of the wound and no crude manipulation of the tissues with the fingers is therefore imperative!
4. The medial circumflex femoral artery is located posteromediad (femoral artery ->deep femoral artery -> medial circumflex femoral artery). Its location and caliber vary greatly, and it often presents with a large caliber. It must be looped separately and clamped later, since injuries to this vessel might result in bleeding that can be hard to manage.
5. In PAOD Fontaine stage IV and during repeat procedures, pronounced adhesions between the femoral artery and the deep femoral vein usually complicate the field. In these cases, time-consuming dissection is to be expected.