Upper abdominal right-angle laparotomy and exploration of the abdomen to exclude an extrahepatic tumor and peritoneal carcinomatosis (not shown). Transection of the falciform ligament down to the level of the confluence of the hepatic veins into the inferior vena cava.
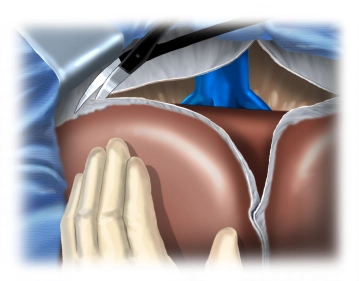
Release of both liver lobes from adhesions with the triangular ligaments, exposing the retrohepatic inferior vena cava.
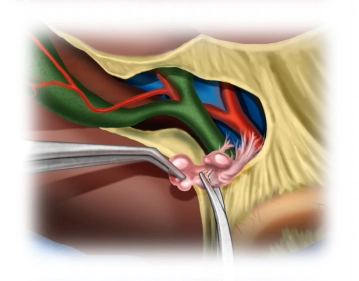
The inferior vena cava is dissected from caudal to cranial, with the smaller distal hepatic veins being gradually exposed. In this case, two larger, variably occurring inferior venous branches are initially transected between Overholt clamps and ligated.
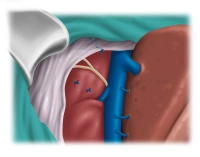
The management of the short central hepatic veins into the inferior vena cava is performed depending on the caliber, using either a clip or transfixion ligature.
Tip: Generous retrohepatic mobilization facilitates resection and prevents blood loss or injury to the vena cava during anterior traction of the liver during parenchymal transection.