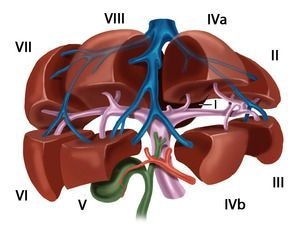
The functional division of the liver is based on the branching of the portal vein into independent subunits called segments.
Portal Vein Anatomy:
- The portal vein typically bifurcates at the liver hilum into a right and left main branch
- The boundary between the territories of these branches is the Cava-Gallbladder line (Cantlie’s line)
- The right branch divides further into an anteromedial trunk (supplying segments V/VIII) and a posterolateral trunk (supplying segments VI/VII)
- The left branch courses transversely to the left and then anteriorly as the pars umbilicalis, terminating at the insertion of the ligamentum teres hepatis in the Recessus rex. It provides branches to:
- Segments II and III (left lateral segments)
- Segments IVa and IVb (left medial segments)
Unique Case of the Caudate Lobe:
The Lobus caudatus (Segment I) is unique as it receives significant inflow from both the right and left main portal branches.
Segmentation According to Couinaud:
The liver is divided into eight portal venous segments, numbered clockwise starting from the caudate lobe:
- Segment I: Caudate lobe
- Segments I/II/III: Left lateral lobe
- Segment IV: Left paramedian sector (Lobus quadratus)
- Segments I/II/III/IV: Left liver lobe
- Segments V/VIII: Right paramedian sector
- Segments VI/VII: Right lateral sector
- Segments V/VI/VII/VIII: Right liver lobe
Hepatic Veins:
The liver is traversed by three main hepatic veins — right, middle, and left hepatic veins — which divide it into four hepatic sectors:
- The left hepatic vein drains the left lateral lobe and usually joins the middle hepatic vein near the vena cava
- The middle hepatic vein follows Cantlie’s line and separates the left and right paramedian sectors
- The right hepatic vein runs between the posterolateral and anteromedial segment
The Lobus caudatus has independent venous drainage through multiple small veins (Spieghel’s veins) that directly empty into the vena cava.
Portal and Venous Hilum:
- The portals of segments II, III, and IV are extrahepatic and can be dissected relatively easily at the anterior portion of the left umbilical fissure
- The portals of right-sided liver segments are intrahepatic, with Segment VI occasionally presenting exceptions
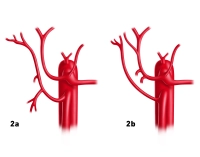
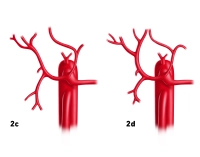
Variations:
Portal Venous System:
- Anomalies of portal vein bifurcation almost exclusively affect the right main portal branch:
- Portal vein trifurcation: The right main branch is absent, replaced by two branches supplying segments V/VIII and VI/VII
- In rare cases, one right branch may arise from the left portal vein
- Variants in the left portal system usually involve segmentation:
- Multiple small branches instead of two distinct branches for IVa/IVb
- Occasionally, an intermediate branch exists between segments II and III
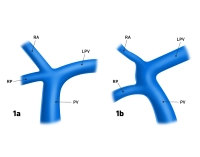
Figures 1a and 1b
- PV = Portal vein
- LPV = Left portal vein
- RA = Right anterior portal vein branch
- RP = Right posterior portal vein branch
Hepatic Veins:
- Variations in hepatic veins are more common than in the portal vein system
- Deviations from Couinaud’s hepatic sectors primarily affect the territories of the right and middle hepatic veins
This detailed knowledge of functional and variant anatomy is essential for precise planning and execution of liver resections.