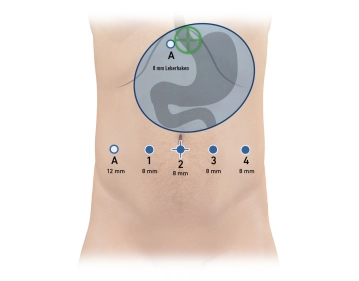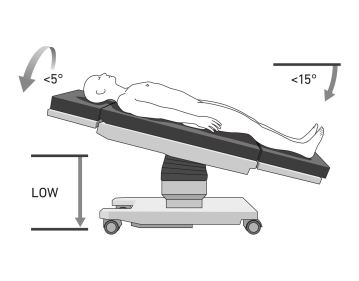
The patient is positioned in supine position on the large vacuum cushion. The left arm can be positioned outwards. By using the cushion, all further supports are omitted. The extremities and all pressure-sensitive areas are padded. A hoop is recommended to protect the patient from the robot arms. After inserting the trocars, the operating table is tilted to approx. 15°-anti-Trendelenburg and approx. 5°-right lateral position (Tilt right).
Caution: The positioning is of particular importance due to the docking of the patient to the robot's manipulator. Risk of injury to the abdominal wall if the patient slips.
Note: Vacuum cushions can have leaks. Check again before sterile draping.
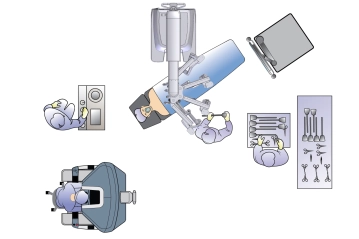
The following setup is chosen: The surgeon sits at the console ideally also with the possibility to look at the patient and table assistant, the table assistant sits to the left of the patient. The anesthesia is located at the head of the patient. The patient cart is approached from the right cranial to the patient and the instrumenting OR nurse is located to the right of the table assistant