

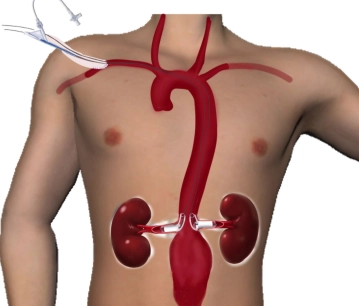
Approx. 8 cm long, slightly oblique skin incision right infraclavicular. Dissection in depth and exposure of the subclavian artery, which is looped with a vessel loop. Clamping of the artery centrally and peripherally, then longitudinal arteriotomy using a stab scalpel and Potts scissors to 8 mm. Sewing in of an 8 mm Dacron prosthesis as conduit access to the artery using Prolene 5-0. Before completion of the suture, flushing. Good inflow and backflow. Completion of the suture. The free end of the prosthesis is ligated with a Mersilene thread. After release of the blood flow, the subclavian artery peripheral to the anastomosis can be well palpated. Puncture of the conduit with a cannula and advancement of a Terumo® wire under fluoroscopic control centrally into the ascending and descending aorta, then advancement of the wire to infradiaphragmal. Insertion of an 8F sheath and administration of 2000 IU heparin.
-
Right infraclavicular access, sewing in of a conduit, probing of the aorta
![Right infraclavicular access, sewing in of a conduit, probing of the aorta]()
Soundsettings -
Bilateral transfemoral accesses, aortic probing
![Bilateral transfemoral accesses, aortic probing]()
Soundsettings In the area of both groins, a 5 cm long skin incision each, preparation and exposure of the common femoral artery. Looping of the arteries using Vessel Loops. Puncture of the left femoral artery using a cannula and advancement of a Terumo® wire under fluoroscopic control centrally. Insertion of a 7F sheath and administration of 2000 IU heparin. Exchange of the Terumo® wire via a pigtail catheter for a rigid back-up Meier® wire. Same maneuver on the right.
-
Probing of the Renal Arteries
![Probing of the Renal Arteries]()
Soundsettings Repeated puncture of the conduit in the area of the right subclavian artery as well as advancement of another Terumo® wire under fluoroscopic control to infradiaphragmatic and insertion of an 8F sheath as well as administration of 2000 IU Heparin. Angiography with visualization of both renal arteries, the superior mesenteric artery and the celiac trunk. Marking of the renal artery origins from the aorta. Careful probing of the left renal artery and then the right renal artery using Terumo® wire. Exchange of the Terumo® wires via vertebral catheter for Rosen wires. Exchange of the left femoral sheath for a 20F sheath and advancement of the same centrally.
Through the two right infraclavicular sheaths, the covered Chimney stent grafts are introduced into
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
US$51.88/ yearly payment
vascular surgery
Unlock all courses in this module.
US$103.80 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.