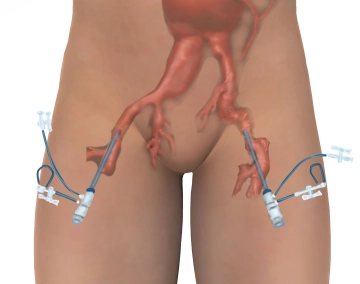
After puncturing both groin arteries, two guidewires are first introduced from the right via a sheath. From the left, a Dormia basket is introduced over a long sheath. This is used to grasp one of the stiff wires and pull it from right to left in the groin over the sheath, so that the wire can be tensioned from both groins to position the endoluminal prostheses in the next steps. Now, the iliac prosthesis part with side arm for the internal iliac artery is introduced from the right with a delivery system, partially deployed, and positioned. Then, probing is performed with a delivery system from the left to advance the extension into the side arm up to the internal iliac artery and deploy it. Next, the iliac prosthesis part is completely released. In a further step, after probing the aorta with a stiff wire from the left femoral, a delivery system with the Y-prosthesis main body is introduced and deployed. Finally, the main body and the left-sided iliac prosthesis module are connected with another tubular prosthesis piece.
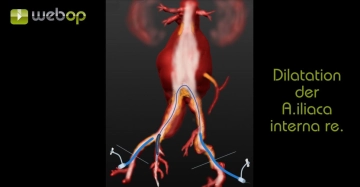
In our case example, various steps were modified because it was necessary to dilate stenoses of the right common and internal iliac arteries. Also, an additional extension was introduced on the left iliac side for surgical tactical reasons.
(Copyright (c) 2015 by W.L. Gore and Associates GmbH. Used with permission.)