

Skin incision approx. 1 cm above and parallel to the clavicle, with orientation at the sternoclavicular joint and at the anterior edge of the trapezius muscle. Division of the platysma. Ligation and division of superficial lymphatic collectors and neck veins.
-
Left supraclavicular access
![Left supraclavicular access]()
Soundsettings -
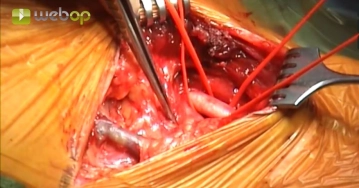
Preparation of the common carotid artery
![Preparation of the common carotid artery]()
Soundsettings Medial to the sternocleidomastoid muscle and the internal jugular vein exposure of the common carotid artery and looping with two vessel loops.
Attention:
Preservation of the vagus nerve! Lesions lead to hoarseness, because the recurrent fibers in the vagus nerve run caudally and only then return to the neck below the aortic arch.
-
Ligation and Division of the External Jugular Vein
![Ligation and Division of the External Jugular Vein]()
Soundsettings Exposure and division of the external jugular vein between transfixion ligatures. Small lymphatic vessels are secured with clips in the supraclavicular fat pad and divided.

Transection of the anterior scalene muscle
Exposure of the phrenic nerve on the anterior scalene muscle. Successive transection of the muscle
Exposure of the phrenic nerve on the anterior scalene muscle. Successive transection of the muscle
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.23 / module
US$50.80/ yearly payment
vascular surgery
Unlock all courses in this module.
US$8.46
/ month
US$101.60 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.