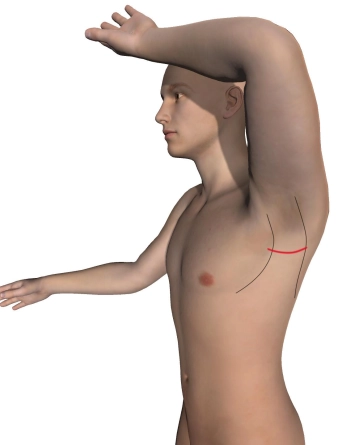
Make a horizontal, curved skin incision in the left axilla over the palpated third rib (usually at the inferior border of the hairline) from the lateral aspect of the pectoralis major muscle to the anterior aspect of the latissimus dorsi muscle. Carry the partly sharp, partly blunt dissection down to the chest wall. Transect the longitudinal lymphatics between ligatures and bluntly sweep away the axillary lymphatic and adipose tissue until the thoracodorsal nerve and long thoracic nerve become visible, as well as the intercostobrachial nerve, which travels from the second intercostal space into the axillary adipose tissue.
Divide between ligatures the lateral thoracic artery and the thoracoepigastric vein, the accompanying vessels of the latter nerve. Insert bladder retractors anteriad at the pectoralis major muscle and posteriad at the latissimus dorsi muscle.
Tips:
1. The transaxillary approach is well suited to clear the first rib with rather good visibility and allows for any needed additional intraoperative procedures (arterial repair, venous thrombectomy and thoracic sympathectomy). Wound healing and the cosmetic outcome of the scar located in the hairy axilla, are generally considered to be very good.
2. If the skin incision is too far superior, access through the adipose and lymphatic tissue of the axilla becomes more difficult.
3. All nerves must be spared and left in place on the chest wall. In other words, do not elevate them with the muscles!