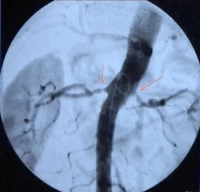
- High grade unilateral or bilateral RAS (>70%) with the aim of organ preservation (see indication in video clip)
- RAS in single kidney function
- Fibromuscular dysplasia of the renal arteries with stenosis and hypertension
- Difficult to control arterial hypertension in RAS
Angioplasty is not indicated in asymptomatic renal artery stenosis (even if bilateral).
In unilateral stenosis and impaired global renal function, the kidney downstream of the stenosis has usually been spared the elevated blood pressure, whereas the kidney with normal arterial lumen has been impaired by chronic hypertension (renin–angiotensin mechanism). Often, renal artery angioplasty of the unilateral stenosis can then improve the function of the poststenotic kidney.
Revascularization of the renal artery is not promising in kidneys with a longitudinal diameter of less than 8 cm and/or proteinuria >1 g/day.
(See also the German guideline Leitlinie - S2K Erkrankungen der Nierenarterie) [Consensus S2 Guideline - Disorders of the renal artery)