Origin
- It is the extension of the thoracic aorta after it passes through the aortic hiatus at the level of 12th thoracic vertebra (T12)
Course
- Retroperitoneal
- Left of midline, anterior to spine
- At the level of umbilicus/4th lumbar vertebra (L4) dividing (aortic bifurcation) into the common iliac arteries
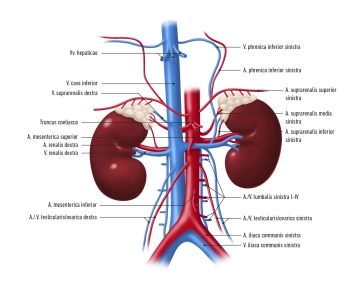
Cephalocaudal branches
- Inferior phrenic arteries
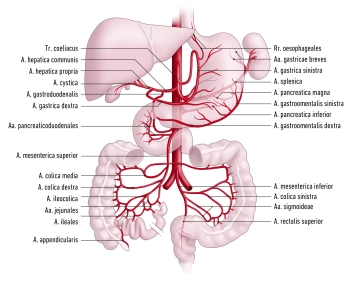
- Celiac trunk
- Left and right middle suprarenal artery
- Superior mesenteric artery
- Left and right renal artery
- Left and right ovarian / testicular artery
- Lumbar arteries
- Inferior mesenteric artery
- Median sacral artery
Arterial blood supply for
- Paired branches: abdominal wall, paired retroperitoneal organs, gonads
- Unpaired branches: spleen, unpaired digestive organs